Before OMG there was om. Negativity of previous posts must be redressed by suggesting a couple of ways to take charge over the body’s natural reactions to an often harsh world. Traditional eastern wisdom has recently been embraced by psychologists and business coaches alike. One can follow a mindfulness franchise on the strength of empirical evidence such as that published by Prof Richie Davidson. ‘Alterations in Brain and Immune Function Produced by Mindfulness Meditation’ , 2003 or ‘A comparison of mindfulness-based stress reduction and an active control in modulation of neurogenic inflammation’, 2013. Bill Malarkey published ‘Workplace based mindfulness practice and inflammation: A randomized trial’ in 2013 but his unfortunate name may prevent it’s being taken seriously. Both studies used Kabat-Zinn’s MBSR as an intervention, although following Vidyamala Burch is made easier by the offered product sample at Breathworks. Ahhh!, the rheumatologist detractors cry, these investigations are predicated on antibody measures and inflammatory markers such as C-Reactive Protein – which we deny being manifest in fibro!
For you skeptics there’s the second, harder path. Let’s start from the premise that FM is a manifestation of a dysregulated cortisol/adrenalin factory – the HPA axis. Deep in our monkey brain is the amygdala which fuels the fight or flight adrenergic pathway, however this is a coarse control since chemical metabolism takes time. Calming electrical override is by the parasympathetic nervous system vagus nerve with help from serotonin-fired neural dopamine fueling a (hopefully) rational prefrontal cortex. Unfortunately, fibro and CFS sufferers lack this moderating instantaneous control as evidenced by reduced heartrate variability. Ashok Gupta’s solution is to re-programme the amygdala. Good luck with that, however evolving tens of thousand years isn’t a promising intervention. <Update Feb 2015: Apologies, Ashok-ji. I’d overlooked December’s report in Arthritis & Rheumatology ‘Overlapping Structural and Functional Brain Changes in Patients With Long-Term Exposure to Fibromyalgia Pain’. The amygdala changes in the right-hand diagram are associated with chronic pain causation…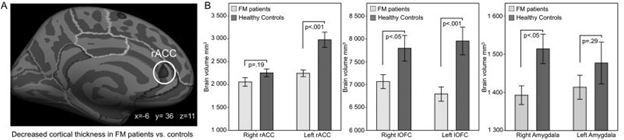
…returning to neuroimmunopharmacology> Parasympathetic neurotransmitter Acetylcholine can inhibit inflammatory InterLeukin-6 (that alone is worth thinking about for its role in TMJD resulting from teeth grinding). Not that you’re going to meditate out of a fever, rather the need is to put the brakes on auto-immune pathways. IL-6 and IL-1 deplete Tryptophan, which we’d all prefer be used in creation of serotonin and ATP for energy but through Tumour Necrosis Factor it’s dumped. It’d be great to block TNF-α upfront through aggressive biological agents such as etanercept or adalimumab, but as rheumatologists deny FM’s suitability this won’t eventuate. Blocking IL cytokines is an even better idea, since Profs Hutchinson and Watkins showed neuropathic pain can be suppressed with naloxone – a shorter acting version of the opioid dependency treatment naltrexone. The diagram in Younger & Stringer et al article: Daily cytokine fluctuations, driven by leptin (tells the hypothalamus to get prolactin out there, but let’s not go there), puts these interactions much more clearly 😉
Analysis, paralysis. The neuroimmunologists and endocrinologists weaving logical arguments is messy theory, but the practice is up to your own mind. There’s so little profit to be made that pharma won’t be sponsoring studies into a quickfix pill – waiting for lowdose naltrexone proponents to capitalize on successes by Prof Younger, with approval to market seems most unwise. A mindful approach is more achievable than your cerebral cortex would think!

Pingback: Impermanence | F'n Myalgia