What does (S)-3-(aminomethyl)-5-methylhexanoic acid do for you? That depends on whether you’re a doctor prescribing Lyrica, a pharmaceutical company making pregabalin, or a patient:

Stop the drug, swelling goes. © Canadian Medical Ass’n
It’s four years since my last incredulous post on the alliance between researchers and Pfizer, a collusion formalized in business collaboration at Monash University in Jun ’17. This revisit begins with the TGA (equiv to US FDA) Product Info for health professionals on Lyrica/pregabalin as of Sept ’16. The first condition of painful Diabetic Neuropathy (PDN) lists 5 completed studies in Table 1, showing pain was halved for ~26% of those administered 150mg, and ~45% if on 600mg. This would encourage doctors to increase dosage up to the maximal 600mg daily (double that allowed in the US). The most frequently reported side-effects are weight gain, dizziness and sleepiness. The manufacturer has checked on driver safety, but research simply doesn’t encompass a thought that harms should be measured systematically: Prof Nadine Attal replied to my concern with “I agree… because the methods used to assess side effects are seldom standardized, particularly as regards cognitive effects of drugs“. This is an obvious pharmacovigilance problem, but another risk lurks. Pg13 of the TGA brochure informs doctors that less than 4% of trial participants suffered peripheral oedema (pictured). None of their advice is referenced, so let’s fact-check.
Peripheral Oedema/swelling
Pfizer reported in ‘A Comprehensive Drug Safety Evaluation of Pregabalin in Peripheral Neuropathic Pain’ that they’d run 13 Randomised Controlled Trials of Lyrica for PDN up to May ’12. Somewhat surprising that the TGA only found 6, which also included independent investigations. Oedema was reported in 9% of neuropathy patients. The manufacturer paints a harms picture that’s doubly worse than the govt regulator does! One Pfizer trial continued for another year with volunteers, of whom 16% reported oedema (10% resolved inside 2 months). Oedema is associated with congestive heart failure, so it matters. And the worsened circulation is associated with non-healing ulcers in diabetics, and that can lead to amputation. Wondering what have you got to lose by starting with this drug – a foot, perhaps? Regardless of adverse events/side-effects, stopping the drug resolves that issue – but at the end of any study there’s limited data captured on withdrawal effects.
Addictiveness
Enriched Enrollment Randomised Withdrawal is a legitimate study design, whereby everyone is dosed and only responders continue into the trial. If it didn’t work for you, goodbye. This means that the group randomized to placebo go through withdrawals, and Pfizer ran this protocol thrice (twice including DPN). After an avg of 400mg daily for a month, then 150mg for one week tapering, pain was marginally worse in the placebo group after a month. 2.5% of the Lyrica group withdrew due to adverse events compared with 6.5% of the placebo arm, hinting at withdrawals suffering. The same protocol with backpain participants finished with both groups reporting the same level of pain, although the withdrawal arm experienced worsening sooner. The endpoint is in accord with the PRECISE study’s finding that Lyrica doesn’t work for backpain.
A lengthier and larger study was run, but this time concomitant meds other than paracetamol were disallowed. Previously patients had continued their own opioids or gabapentin (a Lyrica predecessor), but now the effect of withdrawal was pronounced – some 2 months of worsened pain. Interestingly this study team included Dr Cory Toth *, who’s had 9 papers retracted due to fabricated results. The team then ran a study without Toth, which showed no benefit whatsoever for Lyrica in PDN.

Placebo group suffering withdrawals from run-in period
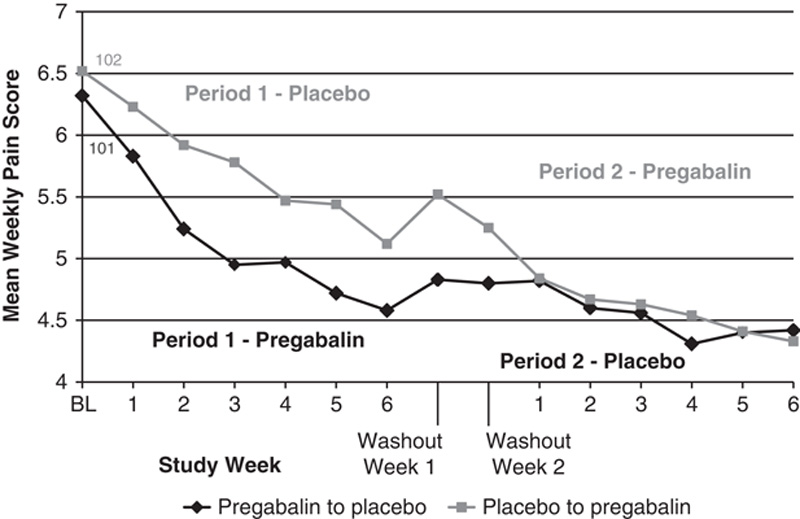
Another protocol requiring drug withdrawal is the crossover design. This study on pre-diabetic neuropathy , again funded by Pfizer, shows a pain spike lasting just 1 week upon switching from drug to placebo.
© 2016 Wolters Kluwer
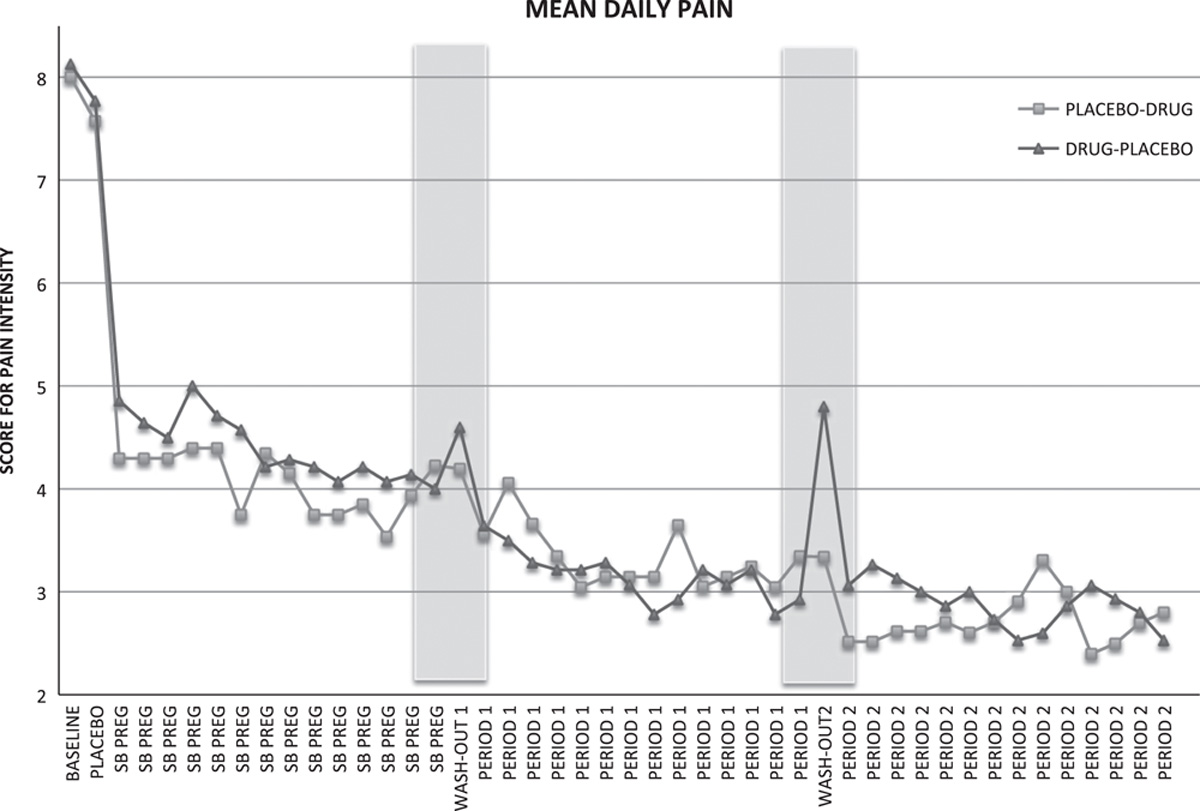
Another PDN crossover study is intriguing – worse withdrawals were suffered going from placebo onto pregabalin in the first week, altho’ actual withdrawals from the drug lasted 3 weeks. Again, the outcome was of a nearly worthless drug, but it’d seem that the fear of losing relief from pain (even if just an imaginary benefit) caused hurtful anguish.
© 2015 Wolters Kluwer
An independent review aggregated 15 trials up until Mar ’16 and concluded …”an overall small effect size with significant heterogeneity in the findings. Reporting bias was a particular concern, due to the high number of unpublished studies.” The 5 TGA examples chosen in their approval decision were an obvious cherrypick of the best results from the picture, being Refs: 17, 18, 19, 21, and 22. It seems that the benefit is arguably small, and data on withdrawals is limited. A recent review on Lyrica’s abuse potential coincides with transfer to Class C schedule in the UK underway, informed by little more than frequent discovery in prisons. Public forums are informative: this group, including recreational users, has a couple of hundred user comments… http://www.bluelight.org/vb/threads/531159-Lyrica-Withdrawal/page8 ** Surprisingly, a ‘comprehensive’ report in Oct ’17 came up with only 4 reported cases of withdrawal symptoms ever, where usage had been within therapeutic guidelines. The gulf of understanding between medicine and its recipients widens. Impressive commentary from the Trump-appointed FDA head on their concern with Lyrica notes that monitoring Bluelight is a gauge of potential for abuse.
Although not the decision makers, patients were treated to $USD344m of Lyrica TV advertising in 2016 (per Nielsen). Half of which was promoting use in diabetic pain. Small comfort can be found in Pfizer’s report that glycaemic control is only fractionally worsened. I do not feel the need to examine every condition for which Lyrica is approved – one instance of systemic failure suffices. For more on the politics of pain, you’d have to ask Chronic Pain Australia’s President or Executive Director as to why they refuse to share this article with their membership: read on…. Geoff Kirwood GDip Clin Research
* Cory apologized, but whether he was ‘sincerely’ sorry is questionable (Confidence Interval bounds not given): “I am significantly apologetic”. His resignation isn’t mentioned on the faculty page, and vice-dean MacQueen accepted his declared failure to oversee his 9 instances of data manipulation. She consults to Pfizer. Scott Reuben went to jail for fraud in 21 papers, which must exceed the threshold of acceptable levels of mistakes. Colleagues Buvanendran and Kroin on Reuben’s retracted pregabalin study went on to publish a favourable study on pregabalin. Paid for by Pfizer. However it doesn’t taint the evidence base, oh no, no, no.
** Bluelight is dedicated to drug harm reduction, and is named after the flame of crystal meth.
