In earlier critiques of Bad Medicine I’d wondered at the contradiction of regulatory authorities handing down $bn punitive fines for wicked off-label promotion of meds, while sponsoring trials that potentially expand the range of approved conditions and thus the on-label market. Part(3) of this series on pregabalin/Lyrica concludes herewith.
In 2011 the Pharmaceutical Benefits Scheme refused Pfizer a subsidy for Lyrica on the grounds that none of the studies thus far had shown efficacy against neuropathic pain. Just 12 months later, they changed their mind. What new data could have influenced this, when the drug’s ineffectiveness was already the source of a joke on its side-effect of dizziness (Schwindel, translated in German)? Significant adverse events of dizziness and somnolence were manifest at the lowest dosage of 150mg consistently in 38 trials ‘The adverse event profile of pregabalin: A systematic review and meta-analysis of randomized controlled trials’ (Zaccara & Specchio et al, 2011).
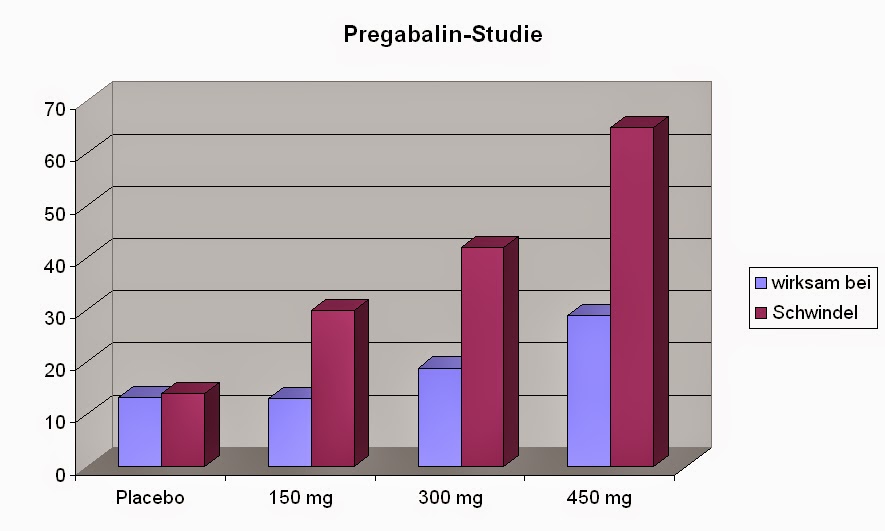
Courtesy of rheumatologist Dr L.Kirsch MD, Jun 2012
This somewhat contradicted Pfizer’s sponsored investigation into Lyrica: ‘Cognitive effects of pregabalin in healthy volunteers’ (Stalinsky, Storzbach & Muniz 2009) offering a conclusion of “… negative cognitive effects and neurotoxicity complaints”. The drug only works (wirksam) to relieve pain at larger doses, at which point there’s been an exponential increase in Schwindel.
Pfizer’s 2012 re-submission to PBAC had two new studies; Boyle, Gribble & Johnsen et al , finding “…there was a significantly higher number of adverse events in the pregabalin treatment group. Conclusions: There was no significant difference in analgesic efficacy between amitriptyline, duloxetine and pregabalin.“, and Trial 1107 – an unpublished, internal study run by Pfizer. I’ll repeat that. The former showed no superiority of the med over amitriptyline, a 50 year-old mainstay known as Endep, furthermore it had worse side-effects. And the in house report …. one can only hope that it was run with more probity that their Trovan trial, best described as a crime against humanity. In summary – this one piece of evidence, from behind closed doors, sufficed to allow “The PBAC recommended an Authority Required (Streamlined) listing of pregabalin (all strengths) for the treatment of refractory neuropathic pain not controlled by other drugs on the basis of acceptable cost-effectiveness compared with placebo in patients dissatisfied with their current pain relief.”
There was another study submitted to PBAC, a comparison showing pregabalin as better than amitriptyline in cancer pain. At a dose of 600mg – at which point conscious state is altered.
What else changed from 2011? Dr Suzanne Hill, co-editor of ‘Evaluating Pharmaceuticals for Health Policy and Reimbursement’ *, was appointed chair of PBAC. This went down well with the pharmaceutical industry. She’s since returned to WHO in the Expert Committee on the Selection and Use of Essential Medicines , replaced with Prof Andrew Wilson per command of Health Min Sussan Ley – who’s been recently forced to resign due to misconduct. I have no idea if governance has improved, nor can inform as to whether it ever existed.
The drug really didn’t work. The 2012 NHMRC grants round allocated $0.62m (plus topups) to try Lyrica for sciatica – leg pain from back nerve damage. Last month PRECISE’s results were posted: no benefit over placebo, and 40% reported the adverse side-effect of Schwindel. Pfizer still won though – they didn’t have to pay for the study. In the interim, the musculoskeletal team of experts had railed against alternative approaches such as imaging – although that’s done with a view to inspecting the problem source for potential intervention at the site. Dr Hill’s colleague at WHO, Prof Lisa Bero didn’t ever respond to concerned memos regarding the probity of PRECISE, nor to complaints about the Monash/NHMRC cases of misconduct.
On the one hand, we trust pharma to do the studies, and on the other, we fund universities to do the studies on their behalf. Win, win for the industry.
*Page 37: “There is evidence that the research methods of trials sponsored by drug companies are at least as good as the trials sponsored by public resources, and in many cases they are better“, referencing Bero – “Study design in drug company sponsored clinical trials better than in research where no stated sponsorship” in her thoughts. My opinion is that trial 1107 should publicly release the names of researchers, or am I asking too much? They’re kept secret, and bound by confidentiality, per NCT00407745: “There IS an agreement between Principal Investigators and the Sponsor (or its agents) that restricts the PI’s rights to discuss or publish trial results”.

This REALLY is the last word from me on Lyrica: https://fnmyalgia.com/2019/01/02/bad-medicine-part-5/
Errata: it goes onBad Medicine (ad finitum)