A few years back I was volunteer non-emergency driver for Red Cross ambulant patients going to clinical appointments. The car was fully booked, and the third for the backseat was my last pickup. They had an an older Left Ventricle Assist Device, with huge powerpack. “Would you all squeeze up on the backseat to make room for the artificial heart?”
Talking to the new client en route to the Alfred’s Heart Failure clinic, ‘Chris’ went to the same Uni as me. Did the same course! I tell my anecdote of mathematician Tom Peachey, how I’d been restoring an old BSA and was tardy in attendance at lectures by this angry little man. “You’ll fail and make nothing of your life, Kirwood“, but I shrugged – I was on my way to 98% … Chris agreed, Tom annoyed him too, “so I slept with his girlfriend“.
Karma. Tom may’ve been ultimately right about me, but Chris sure was heartless!
In the most privileged portion of my career, working at the HyperMed clinic with high level of autonomy in dealing with seriously ill patients, there was a fatality. The deceased, Craig, was stage9 MS, and there is no stage10 *. He’d been rushed to ICU repeatedly, including an airlift from the Latrobe Valley. At the committal for trial pathologist Dr Sarah Parsons claimed cause of death was “Too much oxygen“. The planet certainly would benefit if we evolved to breathe CO2 instead, and I hope her team at Monash are working on this. Sure O2 is a vasoconstrictor, which is why hyperbaric is under pressure of around 30ft underwater – every moist tissue then carries oxygen. And this isn’t quackery – Monash’s physicians at the Alfred hospital also have novel uses for hyperbaric eg adjunct therapy in cancer. Perhaps The Age journo misunderstood Sarah’s evidence (after all, she claimed I had ‘no medical background’ despite the court transcript showing I’ve two decades as a skifield paramedic and a postgrad Dip in Clinical Research)?
Craig also suffered epilepsy. Dr Parson seemingly hasn’t heard that Sudden Unexplained Death in EPilepsy (SUDEP) is actually a thing, despite Prof Chris Semsarian hailing from Sydney and his ‘Post-Mortem Review and Genetic Analysis of SUDEP Cases’ begins: “Sudden unexpected death in epilepsy (SUDEP) is the most frequent epilepsy-related cause of death and is characterized by an absence of any identifiable cause of death…” (Brain Pathology, 2010). And he goes on to point the finger at familial long QT syndrome genes.
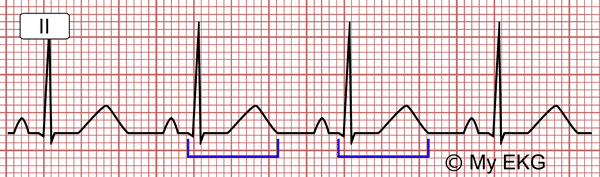
QT-interval-long
The QT interval is the time for the heart’s ventricle to get the signal to pump, and then recharge. Long QT can cause otherwise healthy people to suddenly die, and is the #1 monitoring of concern in ‘first-in-humans’ drug trials. The anti-epileptic drug Lyrica/pregabalin is known to lengthen QT in rabbits, but there’s no data in humans. When Pfizer’s Phillip Berry was asked where’s this key safety info, the reply was Dunno. Yet he received Medicine Australia’s Code of Conduct Award in 2013! Pfizer’s chief pharmacist Manal Nessim also couldn’t help. Cardiologists notice this danger however: Pregbalin induced recurrent syncopal attacks with prolong QT interval – PubMed (nih.gov)
The US FDA’s approval letter of Lyrica for neuropathic pain section Safety Q19 “Has the applicant submitted adequate information to assess the arythmogenic potential of the product e.g., QT interval studies?” is answered NA. And Q25 “Have narrative summaries been submitted for all deaths and adverse dropouts?” is answered No (will request from sponsor).
Craig was on many drugs, including Lyrica. But the chiropractor killed him, right everyone?
* Stage classification is now obsolete.

A message from the Lord:
I wrote the UK Health Min with responsibility for drugs & industry, and Lord James O’Shaughnessy graciously gave me 2 pages of assurance that the cardiac safety data was captured by adverse event reporting. But no, there’s no quantitative QT data on file. Pfizer did collect such, sponsoring a study by Dr Beydoun and providing 3 staff (Kugler, Knapp, and Garofalo), however it stonewalls requests for release. This will be a drawn-out process. Geoff