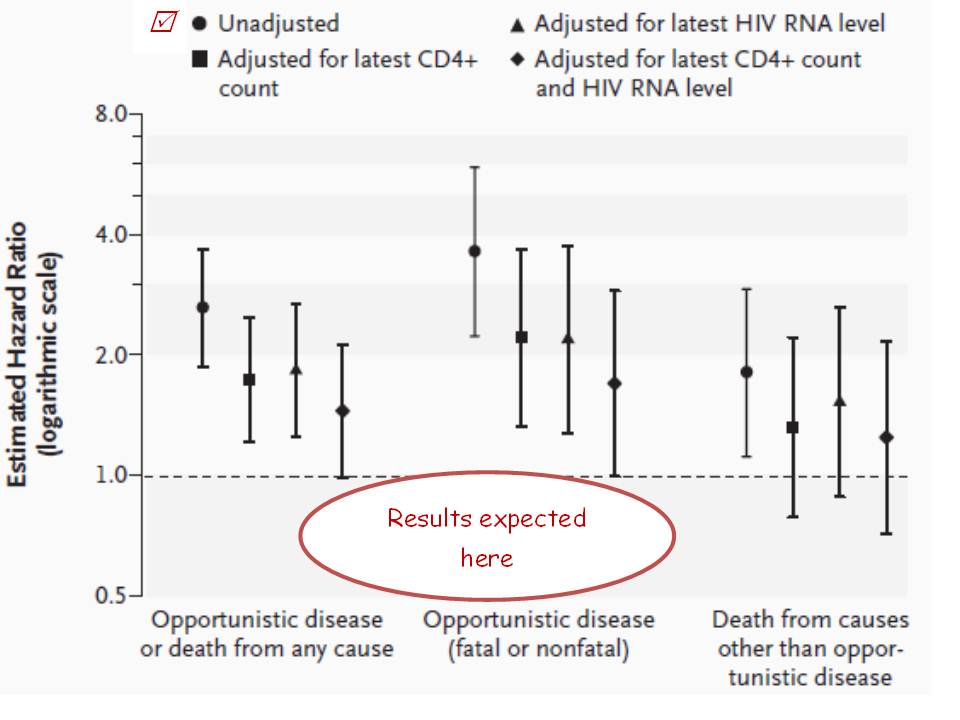
PRO-logue. It’s telling that an identical German study to PRO-HEART was shutdown early. Comments by psychiatrist Andreas Ströhle and Nina Rieckmann from their Institute of Public Health : “Dr Angermann and colleagues reported that escitalopram did not reduce all-cause death or hospitalization… It is not clear why the authors expected that it would, as it does not reduce mild to moderate levels of depression… Rather, it adds to the mounting evidence that questions the risk-benefit ratio of prescribing antidepressants to patients with less than severe depression.”
Once upon a time, psychs drew a distinction between depression originating from within (endogenous) or that which arose due to circumstances (reactive). The former was treated by meds, but the market for anti-depressants has grown as the two-type concept has fallen out of favour. Pills manipulating neurotransmitter levels are a simple solution with scrip from your GP, one that doesn’t require psych expertise. The American Psychiatric Association aren’t blameless, since the criteria for mental illnesses is loosened with every release of the DSM. That manual has also expanded in order to inform practitioners of the complexity of the complex. But they have lost control in this non-infectious pandemic. Prof Peter Gotzsche is fanatical in advocating that prescriptions of such meds be reduced 50-fold, but for a less emotive perspective I suggest you follow psychiatrist Professor David Healy, or read his ‘Pharmageddon’.

Followon book to ‘Deadly Medicines and Organised Crime’
Earlier posts have complained at the fabricated conclusion that chronic pain is manifestation of a mental illness. It was a researcher’s invented report that then conveniently led into a publicly funded trial for anti-depressants in osteoarthritis. It’s to the Royal Aust & NZ College of Psychiatry’s credit that their submission against Medicine Aust code-of-misconduct application to regulatory authority ACCC was the only one to address perversion of research by industry. If they’re to be believed, academics are corrupted. And if Gotzsche is right, you can’t trust Patient Organisations for … “having done absolutely nothing to stop the blatant abuse of patients in industry-sponsored trials“, citing Dr Ben Goldacre’s book ‘Bad Pharma’ of 2012. It’s worse than that, as you’ll find out.
Heart Foundation Vic CEO Jennifer Johns has earlier come in for ridicule over statins, echoing her disgraced NSW President’s associations with the refined sugar industry. An Austin hospital cardiologist, in 2010 she funded her colleague David Hare and Baker IDI’s Prof Krum to trial Lexapro as treatment for the depression that their heart failure patients are presumed to suffer, PRO-HEART. Also in this year the manufacturer’s promotion of such off-label usage cost them $USD313m in fines, with civil actions continuing. Such as 03-10395-NMG for wrongful dismissal of sales rep and whistleblower Chris Gobble, who complained to supervisors of “illegal kickbacks (i.e. paying doctors for no other reason than to induce them to prescribe Celexa and Lexapro)”. The marketing budget disclosed in the Confidential plan provided to the US Senate was $35m on speakers fees, and $36m on lunches. In one year. In one country.
The drug is also associated with hyponatremia, ie it worsens heart failure risk. None of the team answered this concern, but they were defended by the Heart Foundation’s Deidre Cope: “In regard to its Research Program, the Heart Foundation follows the NHMRC guidelines around disclosure of interest. The research funded by the Heart Foundation undergoes a rigorous peer review process involving assessment by independent, external reviewers. All funding decisions are scrutinised by an external committee to ensure that all aspects of the peer review process are consistent, transparent and ethical.” Affirming that they’re just as utterly corrupt as the NHMRC, as evidenced by Cicuttini and Wluka’s impunity.
The other half of the $820,000 raised by door-knockers and tin-shakers that PRO-HEART is costing was from Beyond Blue. No responses to approaches were provided at all. It’s too early to allege misconduct – the trial is running three years behind schedule, and a staffer thought late 2017 would see a report released. But it already stinks like something’s died. [Sep 2017 update: 2018 perhaps? BB CEO Georgie Harman states that she’s happy with the study progress – seven years after the first patient was enrolled in the 6month study]
There’s often a trite closing disclaimer in articles that if you suffer from depression, there’s phone support available at these numbers…… who’ll suggest medical advice. I’m more of the opinion that you think carefully, so have linked further material on happiness or absence thereof at http://themindfulgap.com.au/2016/02/05/the-blue-bird-and-the-black-dog/

 Cochrane pioneers Gotzsche and Chalmers are much alike in their evidence fudging. The
Cochrane pioneers Gotzsche and Chalmers are much alike in their evidence fudging. The 