Martin Seligman’s 2018 ‘The Hope Circuit’ is his autobiographical account of the field of Positive Psychology’s (PP) evolution. As a popularly elected President of the American Psychology Ass’n (APA), despite being unpopular with legacy professorial clinicians, his object was usurp of the American Psychiatric Assn’s cornerstone: mental disorders. This other APA manages the Diagnostic & Statistical Manual (DSM), which establishes thresholds of ‘what’s normal’ in behavior and perception. The DSM pigeon-holes us, much like the museum pins taxonomy labels on insects, but PP refutes the idea of correcting faults. Better that we play to strengths, and let the defects be.

Nailed to a diagnosis
The last chapter is his epiphany – in his seventies, he realizes that he’s been wrong all along. His theory of learned helplessness had been proven in the labs – beat an animal down with inescapable suffering, and they’ll lose the will to fight their way out of the predicament. But his colleague Steve Maier turned that upside down. Our vulnerable infants are nurtured through their helplessness, but based upon success against adversity they build a neural circuit, simple neuroplasticity, that gives resilience. I repeat: we learn to thrive from achieving, else feebly succumb and remain dependent for life.
To be fair to Marty, the neuroscience had only recently matured so as to enable Maier & Watkins’ breakthrough. Though the seminal work is a dozen years old, it’ll be awhile yet before its significance drives psychotherapy dinosaurs into extinction. My personal enthusiasm is kindled by Linda Watkins’ other, amazing insight into fibromyalgia, where along with Prof Younger and Adelaide Uni’s Prof Mark Hutchinson this autoimmune disorder was attributed to the brain’s innate defence mechanism – glial response to perceived viral attack* . Sufferers can’t yet take comfort from that breakthrough, there’s more Randomised Control Trials of an anti-viral combo (IMC-1) to be done over many years.
Back to the ‘hope circuit’. By default the brainstem’s DRN produces serotonin, which calms down the ‘fight or flight’ sympathetic nervous system – but also amplifies anxiety driven by the amygdala in the limbic system. I’ll re-word that for emphasis: serotonin treats panic attacks, but worsens fear. One could ponder the backlash of research, through the likes of David Healy’s Rxisk.org, asking why antidepressants that elevate serotonin have side-effects such as increased suicidality. The simple ‘chemical imbalance’ theory has been thrown out awhile ago (don’t get me started as to whether bloods to review serotonin levels in patients should be analysed, before being handed the happy pills on a presumption of necessitating boost via an SSRI), because we’re not machines but rather systems. Tinker with one process and another will compensate. All this isn’t in the pharmaceutical company brochures, though it’s been well-known for two decades. And the growth market is for teenagers, despite halting the formation of circuits required for later resilience.
DRN hijack of emotions is dampened by previous cognitive rewards from the Pre-Frontal Cortex (PFC, the learning brain) using successful control over situations to increase kinase proteins – described as an ‘immunization’. In animal models the dissected brains are tested for a change to successfully build resilience, and in the last few years studies have been designed for humans using fMRI. Do-it-yourself at home is a no-brainer. PP gives all the tools you need to focus on success, and protect your brain: simply do the survey to ascertain strengths, then determine how best to use them. If that fails, then seek professional help… being prescribed an anti-depressant isn’t the worst possible outcome from a trip to the doctor – script for Lyrica holds that ignominy.
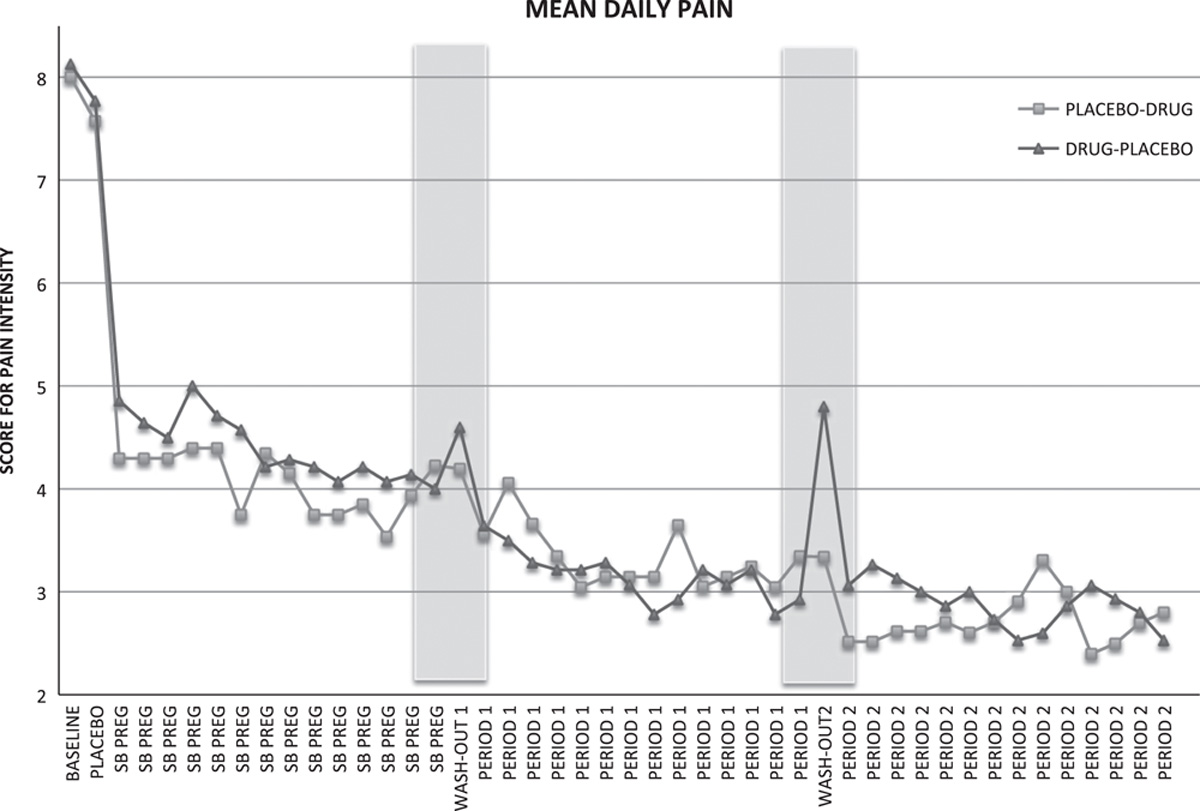
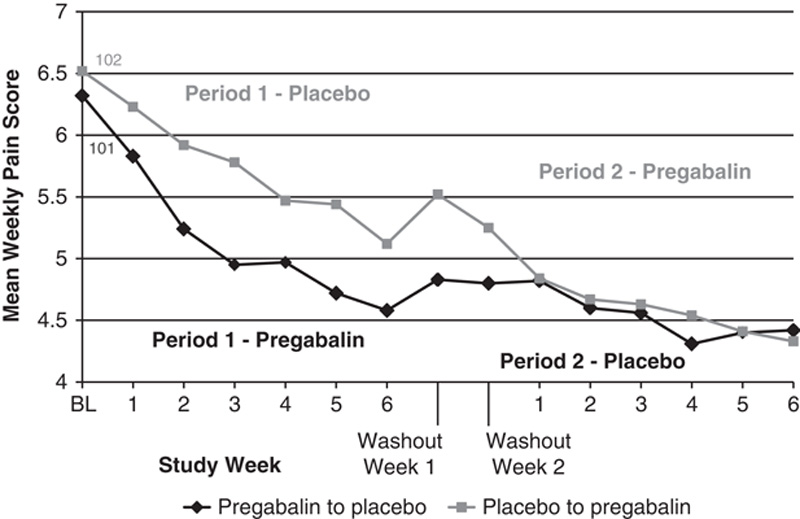
The 2009 Stanford study damning Lyrica as blocking formation of new synapses, connections between neurons, has been cited a further 245 times. The most recent further investigation ‘The α2δ-1–NMDA receptor coupling is essential for corticostriatal long-term potentiation and is involved in learning and memory’ describes how gabapentinoids break the hope circuit (nasty biochem, but Lyrica and Neurontin are designed to block α2δ-1 Calcium subchannels, and the PFC pathway to moderate the DRN is via ERK->NMDA Calcium channels. Please don’t ask for an explanation).
This fresh knowledge has no commercial application, PP will never be packaged in a pill (picrotoxin is used in research as an ‘anti-gabapentinoid’ to artificially create PFC->DRN control, but is deadly!). Worse, the accreditation Master of Applied PP is only taught in Australia at Melbourne Uni – where it’s sequestered away in the School of Education, not Health. An inceptual program is underway centred on Heathmont College, which follows Geelong Grammar’s wonderful work. It’s unlikely that the medical industry’s stranglehold on wellbeing will loosen without generational change through these schoolkids achieving professorship. TheMindfulGap was a partnership with my then wife, doing all we could to prepare the way for chronic illness sufferers to escape helplessness. Hopefully someday someone’s children will value those efforts.
Good luck in the meantime, Geoff
* So what? Well to measure societal suffering through subscribers to forum PatientsLikeMe.com, where the medically disenfranchised seek answers to their condition, 106 thousand fibromites vastly outnumber Major Depressive Disorders 2:1, or backpain 100:1, or arthritics 4:1. Great research tackles great problems.






 Managed by qualified dogcatcher Bernie Shakeshaft, their modus operandi is to attend a rural court where juvenile offenders have run out of warnings, and are due for detention. An alternative offer is made for these feral kids to voluntarily labour on a remote farm, where they’ll also be taught to handle dogs. This goes down well with the Magistrate “… if I can forward them to a structured program like BackTrack, I certainly feel like there would be less recidivism.” In 2013 while Bernie’s brother, University of NSW (UNSW) Prof Shakeshaft, was on the NHMRC council their grant application “This study quantifies the benefits/costs of combining cognitive-behaviour therapy with a community-reinforcement strategy to reduce substance-related harms among young Indigenous Australians” was approved for $386771. A year later Bernie took off on a study tour of the USA, Canada and Italy. Bernie’s been done for Driving Under the Influence, so has learnt by experience the perils of alcohol abuse. But he’s naïve about CBT, and the majority of incarcerated kids aren’t Indigenous. This is revealed in a book submitted by Helena Pastor for her PhD by observation from the local Uni. An excerpted page
Managed by qualified dogcatcher Bernie Shakeshaft, their modus operandi is to attend a rural court where juvenile offenders have run out of warnings, and are due for detention. An alternative offer is made for these feral kids to voluntarily labour on a remote farm, where they’ll also be taught to handle dogs. This goes down well with the Magistrate “… if I can forward them to a structured program like BackTrack, I certainly feel like there would be less recidivism.” In 2013 while Bernie’s brother, University of NSW (UNSW) Prof Shakeshaft, was on the NHMRC council their grant application “This study quantifies the benefits/costs of combining cognitive-behaviour therapy with a community-reinforcement strategy to reduce substance-related harms among young Indigenous Australians” was approved for $386771. A year later Bernie took off on a study tour of the USA, Canada and Italy. Bernie’s been done for Driving Under the Influence, so has learnt by experience the perils of alcohol abuse. But he’s naïve about CBT, and the majority of incarcerated kids aren’t Indigenous. This is revealed in a book submitted by Helena Pastor for her PhD by observation from the local Uni. An excerpted page 